Thanks for your great tool! I'm a newbie to SEEG analysis. I have raw T1w, CT images, and SEEG data in EDF format. And I use Brainstorm for electrode localization and labelling all contacts using the AAL3 atlas.
After reading the tutorial and practising the localization process, I have some basic questions about the usage of brainstorming for SEEG electrode localization.
MRI segmentation seems to do a lot, but in my case, I understand that it is primarily used for MNI normalization and for the atlas labelling of contacts. Currently, the main methods for normalization include mff8a, spm12, and cat12 (cat12 normally has higher accuracy). Is that correct?
For coregistration, there are currently mainly two methods available: one is ct2mrireg, and the other involves right-clicking on the CT and selecting "register with default MRI -> spm " Is that right?
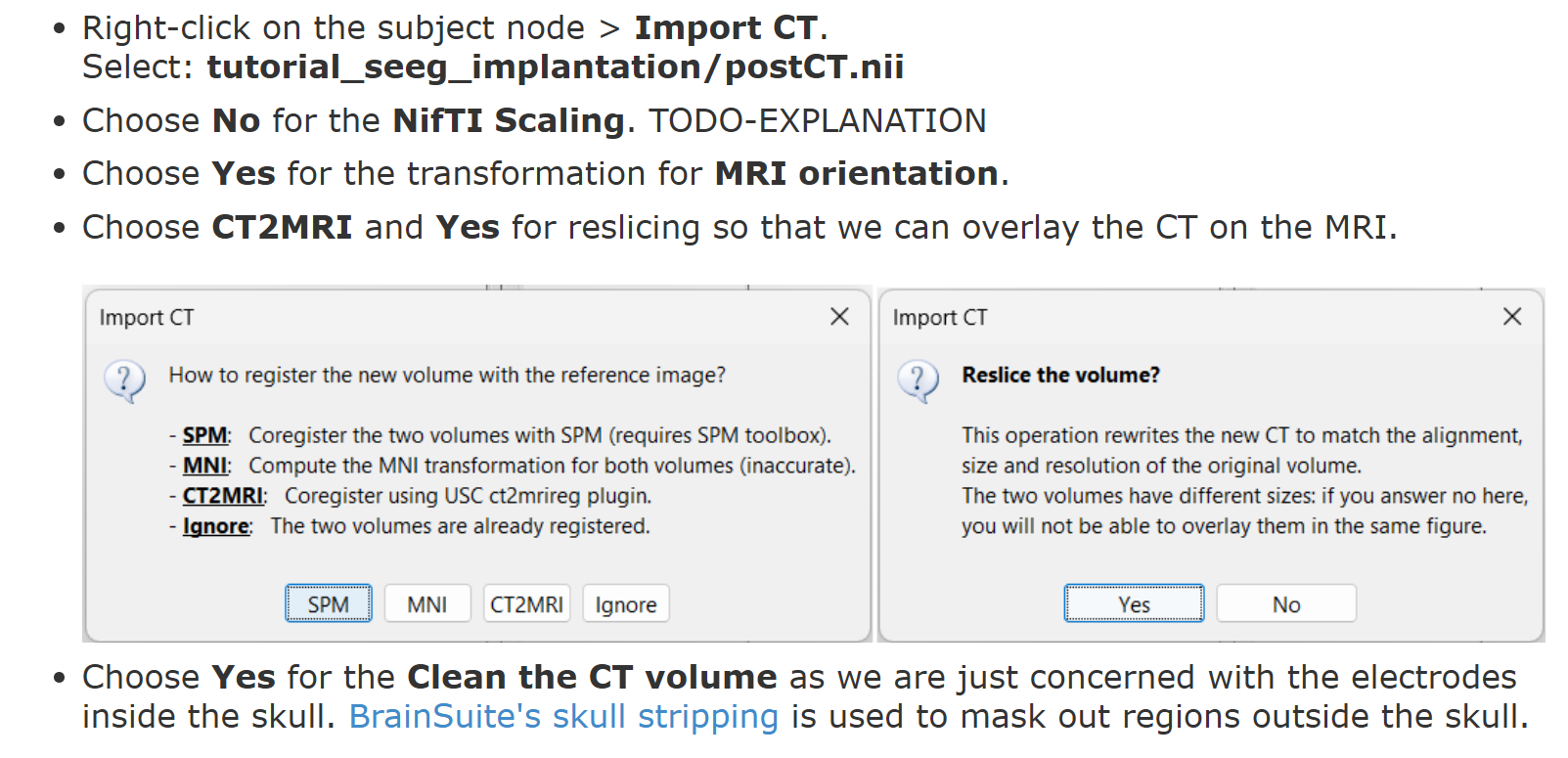
When importing the CT scan, I encountered three pop windows (like the following tutorial) in sequence. I would like to know what the differences between orientation, registration, and reslice are.
Following question 1, I want to know is there any way to reduce the consuming time of CAT12 since I may only use a small part of their results (I'm not familiar with CAT12 so I'm not sure whether things like cortex/tissue/ surface-based processing are necessary for the non-linear normalization here. It would be great if you could explain it more.)
Yes these are the two options available. But we would recommend using the ct2mrireg as it is well validated for registering a CT to an MRI.
Orientation: Check this dicsussion MRi image orientation. Registration: Here it refers to aligning the CT to the MRI to minimize the shifts between them. Mode details can be found here and also in this discussion. Reslice: rewriting a new volume (here, CT) that matches voxel-by-voxel the reference volume (here, MRI). More can be found in this discussion
Thank you for your patient reply! I still have some novice questions about them.
My understanding is that orientation is more like changing the "view" of the CT in Brainstorm, and the corresponding "transformation" is mainly to help Brainstorm recognize the directions like left/right, posterior/anterior, etc. of the CT, right?
Is reslice similar to the resample in other fMRI programs? I don't quite understand why it is done at the end of the process.
I noticed that BrainSuite can also perform segmentation, and ct2mrireg requires calculations in BrainSuite. I would like to know if using BrainSuite for segmentation could save some time in subsequent coregistration. In terms of segmentation accuracy, would you recommend BrainSuite or CAT12?
MRI segmentation with BrainSuite and CAT12 take more or less the same time (approximately 1hr)
Which is fast compared with other MRI segmentation software. Also, this is needed only once per Subject, and can be pre-processed in batches.
Unfortunately, calling CAT12 from Brainstorm implies the entire pipeline.
You may want to check the CAT12 documentation if you only need the non-linear normalization https://neuro-jena.github.io/cat/
Currently, I manually process each subject individually. Every time I import an MRI, I need to manually locate NAS/LPA/RPA and AC/PC/HI points, followed by CAT12 segmentation. I would like to know how to batch-process this localization.
Also, I noticed that the tutorial at ImportAnatomy#MNI_normalization mentions that NAS/LPA/RPA localization can be done automatically (in practice, all six points can be automatically located).
However, I don’t fully understand why these fiducial points are necessary, what subsequent operations they serve specifically, and what the difference between manually located points and automatically calculated ones is. Could you explain this briefly? Thank you!